Colorectal Cancer
Colon and Rectal Cancer
Dr. Cheryl Lau
Dec 3, 2024
Colon and rectal cancer (also known as colorectal cancer) is the most common cancer in Singapore. The colon and rectum are parts of the bowel, and most cases occur in people over 50. If diagnosed early, bowel cancer has a good chance of being cured. In general, the more advanced the cancer, the less likely treatment will be curative, though it can often slow its progression.
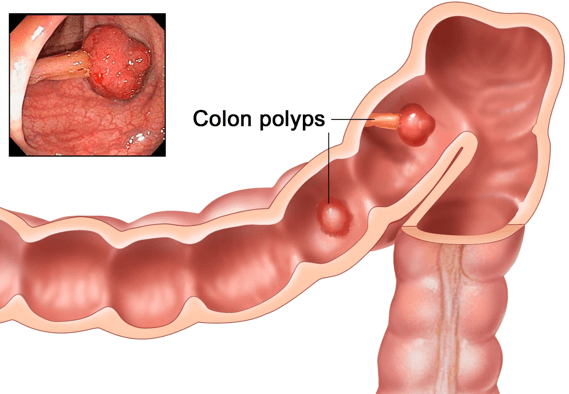
Colorectal cancer can affect any part of the colon or rectum, though it most commonly develops in the lower parts, such as the descending colon, sigmoid colon, or rectum. It usually starts as a fleshy growth (polyp) on the lining of the colon or rectum. In some cases, colorectal cancer begins from non-polyp cells that mutate and become cancerous.
There are also rare types of cancer that can arise from other cells in the wall of the colon or rectum, such as carcinoid tumors, lymphoma, and sarcomas. As the tumor grows, it invades deeper into the walls of the colon or rectum. Cancer cells may break off into nearby lymph channels or blood vessels, spreading (metastasizing) to nearby lymph nodes or other areas of the body, most commonly the liver and lungs.
What Causes Colorectal Cancer?
Risk factors include:
Age: Colorectal cancer is more common in older individuals. Eight out of ten patients diagnosed are over 50. Recently, there has been a concerning trend of colorectal cancer in younger patients.
Family History: If a close relative (first-degree relative) has had colorectal cancer, the risk is higher due to genetic factors.
Personal History: A history of colorectal, breast, uterine, or ovarian cancer increases the risk. Those who have had colorectal cancer may develop it again, so regular follow-ups are important. Women with a history of ovarian, uterine, or breast cancer may also be at higher risk.
Genetic Conditions: Conditions like familial adenomatous polyposis (FAP) or hereditary non-polyposis colorectal cancer (HNPCC) increase the risk, accounting for about 5% of all cases.
Inflammatory Bowel Disease: Conditions such as ulcerative colitis or Crohn’s disease, especially if they’ve been present for more than 10 years, increase the risk.
Obesity
Lifestyle Factors: Smoking, alcohol consumption, and lack of exercise.
Diet: A diet high in red meat, processed meats (like luncheon meat, ham), and processed foods.
A balanced diet with regular intake of fresh fruits and vegetables can help reduce the risk of colorectal cancer.
Colorectal Cancer Symptoms
Early colorectal cancer often doesn't cause symptoms. In its early stages, cancer is too small to block the colon or cause noticeable bleeding. As the cancer grows, symptoms may vary depending on the tumor's location.
Common Early Symptoms:
Bleeding: Blood in stools, sometimes turning them dark. The bleeding is usually mild and may be mistaken for hemorrhoid bleeding.
Chronic Bleeding: Can lead to anemia, causing fatigue and pale skin.
Mucus in Stool
Change in Bowel Habits: Alternating between constipation and diarrhea.
Incomplete Emptying: A feeling of not fully emptying your bowels after a movement.
Abdominal Bloating and Pain
Advanced Symptoms:
More Severe Symptoms: The symptoms above, but more pronounced.
General Malaise: Feeling unwell, tired, or weak.
Unexplained Weight Loss
Blockage: A large tumor can block the colon, causing severe pain, inability to pass stools, nausea, and vomiting.
Perforation: The cancer may cause a hole in the colon or rectum wall, leading to severe pain, life-threatening fever, and fecal leakage into the abdomen.
Metastasis: If cancer spreads to other parts of the body, additional symptoms will depend on where it has spread.
If you experience any of these symptoms, contact a doctor for an evaluation.
Assessment and Screening
Colorectal cancer can often be detected early and even prevented. The most important step in prevention is regular screening. Adults aged 45 or older should undergo routine colorectal cancer screening, and those with close family members who have had colorectal cancer should start screening earlier.
Most colorectal cancers develop from polyps. A colonoscopy, which involves inserting a lighted flexible tube into the colon under sedation, can detect and remove polyps. Identifying and removing pre-cancerous polyps during the procedure can significantly reduce the risk of colorectal cancer.
Other Screening Options
In addition to colonoscopy, other screening options for colorectal cancer include:
Stool Tests: These include stool occult blood tests, fecal immunochemical tests (FIT), and other types of stool analysis.
Flexible Sigmoidoscopy: This is a partial colonoscopy using a shorter scope to examine only part of the colon.
Barium Enema: An X-ray procedure that involves filling the colon with a contrast dye to detect abnormalities.
Virtual or CT Colonography: Used in rare specific situations, but not recommended for routine screening. Any abnormal screening test should be followed by a colonoscopy for confirmation.
Blood Tumor Marker Test
Carcinoembryonic antigen (CEA) is a tumor marker test used in selected situations. However, it is not reliable for diagnosing colorectal cancer because many patients with colorectal cancer have normal CEA levels (false negatives). The definitive diagnosis of colorectal cancer is made through laboratory analysis of tumor tissue (histopathology).
What Happens Once Colorectal Cancer is Diagnosed?
Once diagnosed, the next step is to determine the cancer stage, which is critical for planning the best treatment strategy. Staging describes the aggressiveness and spread of the cancer and is based on:
Imaging tests such as CT scans, MRI of the chest, abdomen, and pelvis, chest X-rays, or PET (positron emission tomography) scans to detect cancer spread.
The cancer specimen viewed under a microscope after removal through surgery.
Baseline blood tests, including complete cell counts (to check for anemia) and CEA tumor marker levels, which can help detect cancer recurrence during follow-ups if raised.
Colorectal Cancer Stages:
Stage I: Cancer has invaded into, but not through, the entire wall of the intestine.
Stage II: Cancer has invaded through the entire wall of the intestine, but no lymph node involvement.
Stage III: Cancer involves the lymph nodes, regardless of whether the intestine wall is affected.
Stage IV: Cancer has spread (metastasized) to distant organs, such as the liver or lungs.
How is Colorectal Cancer Treated?
The primary treatment for colorectal cancer is surgery. The optimal treatment approach depends on the stage of the cancer and its location within the colon or rectum.
Early Stages (Stages I–III): These are considered localized colorectal cancers and are typically treated with surgery, with or without chemotherapy. For locally advanced rectal cancer, radiation therapy combined with chemotherapy is often used to shrink the tumor before surgery.
Stage IV Cancer (Advanced Colorectal Cancer): This is usually managed with chemotherapy. Some patients may benefit from surgery to remove the primary tumor, particularly if it is causing symptoms, before undergoing chemotherapy.
How is Surgery Performed?
Surgery involves removing the segment of the colon containing the tumor, along with the feeding vessels and surrounding lymph nodes. A thorough check of the abdomen is also performed to ensure that the cancer has not spread.
Traditionally, colorectal cancer surgery was performed through large open abdominal incisions using standard instruments. However, minimally invasive surgical techniques, such as laparoscopy or robotics, are now used depending on the patient's condition. In these methods, small keyhole incisions are made in the abdomen. A lighted camera (laparoscope) connected to a video screen is used to see inside the abdominal cavity, and the procedure is performed using specialized laparoscopic instruments.
Research has shown that both open and minimally invasive surgeries yield equivalent long-term cancer outcomes. The choice of approach depends on the individual patient’s situation, and we will discuss these options with the patient prior to the operation.
When a section of the colon is removed, the surgeon will typically reconnect the healthy ends of the colon. This connection is called an anastomosis. Factors such as smoking, steroid treatments, and high blood sugar (diabetes) can impair the healing of this connection, leading to a potential leak of bowel content into the abdomen. In some cases, anastomosis may not be safe, and a new path for waste to leave the body will need to be created. This involves making an opening (stoma) in the abdominal wall to connect the intestine to the skin. A stoma bag fits over the stoma to collect stool waste. When properly cared for, the stoma bag is odorless and easy to manage, thanks to a special adhesive that keeps it in place. The creation of a stoma is typically only necessary for a small number of colorectal cancer patients.
The time it takes to heal after surgery varies for each patient. Discomfort is common in the first few days, and many patients experience fatigue or tiredness. Bloating and changes in stool consistency are also common post-surgery, but we provide guidance on managing these symptoms. Our team will monitor for signs of bleeding, infection, or any potential complications that may require immediate attention.
After discharge, light physical activities, such as walking, are encouraged to aid recovery. Patients should avoid heavy lifting for a certain period to reduce the risk of developing a hernia at the incision site. Generally, a low-fiber solid diet is recommended during the recovery period.
What Other Treatment is Required for Colorectal Cancer?
If colorectal cancer has spread to nearby lymph nodes (stage III) or distant areas (stage IV), chemotherapy is usually recommended. Some patients with early-stage colorectal cancer and certain risk factors may also benefit from chemotherapy. Chemotherapy uses anticancer drugs to kill cancer cells and improve long-term survival by reducing the risk of cancer recurrence in patients with stage III cancer.
Anticancer drugs are generally administered through a vein, though some may be given orally. The most common chemotherapy drugs for colorectal cancer include 5-fluorouracil (5-FU) and oxaliplatin. Chemotherapy may also be combined with targeted therapy drugs, such as bevacizumab or cetuximab, especially for stage IV patients.
Chemotherapy typically begins several weeks after surgery. The side effects of chemotherapy depend on the drugs used and the dosage. Common side effects include fatigue, weakness, increased risk of infections, nausea, diarrhea, mouth sores, and numbness or tingling in the hands and feet. There are ways to manage many of these side effects, and most side effects subside after treatment.